Melanoma

General Information
As chronicled in Steinbeck’s famous novel, the best conceived plans can go awry as in the examination of melanocytes by frozen section pathology. Sub-optimal preservation, freeze artifact, overlapping histologic criteria between melanocytes and confusion with other resident epidermal cells may all conspire to render the evaluation of these lesions problematic. For these reasons as well as the practical concerns of jurisprudence and affording the best technique for the evaluation and treatment of these neoplasms, discussion will be limited to the adjudication of incidental nevocellular nevi and melanoma-in-situ. It is the opinion of this author that dysplastic or other atypical nevi including Spitz nevi and invasive melanoma are best assessed through traditional histological techniques and that the treatment of invasive melanoma should concern wide local margin excision with permanent section margin assessment. Incidental nevocellular dermal aggregates are commonly encountered in the examination of frozen sections of cutaneous neoplasms. The nevic rests can be seen anywhere within the dermis particularly in peri-follicular locales. The nevi themselves typically form loose clusters and are comprised of a uniform population of rounded cells with scant eosinophilic cytoplasm containing rare melanin pigment. The nuclei are typically round and may contain cytoplasmic pseudo-nuclear inclusions. Melanoma-in-situ is most commonly encountered in the setting of chronic actinic damage on the head and neck or exposed extremities clinically configured as the Hutchinson’s freckle or lentigo-maligna. The melanocytes comprising these lesions may be configured as subtle haloed-single cells along the dermo-epidermal junction or entail inter-follicular skip areas with transfollicular extension. Classic criteria of melanoma-in-situ consisting of melanocyte nesting along the dermo-epidermal junction, contiguous basilar layer proliferation and pagetoid scatter should be sought after as important features of these neoplasms. Among the more difficult tasks for the microscopist is the discernment of individual atypical melanocytes in conjunction with solar-induced hyperplasia/hypertrophy and their distinction from other resident cells that possess similar cytologic features. While the average of 1 melanocyte per 10 keratinocytes may exceed a numerical factor of 1 melanocyte per 5 keratinocytes in sun-damaged cutaneous sites such as the face, melanocyte numbers exceeding this ratio, situated as contiguous runs of two or more adjacent melanocytes or showing interfolliclar extension should be regarded as suspicious for melanoma-in-situ. Although Langerhans cells and Merkel cells can be seen along the dermoepidermal junction and can possess pericellular halos as observed with melanocytes, they typically exist in lower numbers on the face or in areas that have received excessive ultraviolet exposure. Another pitfall concerning the histologic assessment of abnormal mel
Epidemiology
Common
Etiology
Pathogenesis
UV light, PF53, C- kit, p16 genetic defects.
Clinical
Irregular hyperpigmented patch on sun-exposed site.
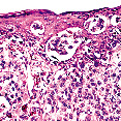
Histology
Bibliography
1. Flotte T. Malignant melanoma in situ. Hum Pathol 1990; 21: 1199. 2. Agarwal N, Bowen G, Gervels J. Histologic assessment of lentigo-maligna with permanent sections: Implications regarding current guidelines. JAAD 2002; 47: 743. 3. Shabrawi L, Kerl H, Cerroni L. Melan-A is not helpful marker in the distinction between melanoma in situ on sun damaged skin and pigmented actinic keratosis. Am J Dermatopathol 2004; 26: 364.
Download PDF
![]() Melanoma
Melanoma