Squamous Cell Carcinoma
General Information
Squamous cell carcinoma (SCC) is the second most frequent form of skin cancer superseded by only basal cell carcinoma. Like basal cell carcinoma, SCC is predisposed for by excessive ultraviolet exposure hence its association with advancing age and cumulative sun exposure, exposed anatomic sites and highest incidence in sunny geographic locales. The most important pathogenic mechanisms involve aberration of the p53 tumor suppressor gene via ultraviolet-induced mutation or HPV-encoded interdiction. The latter mechanism is thought to be the most important factor in the development of these malignancies in the setting of epidermodysplasia verruciformis and solid organ iatrogenic immunosuppression where multicentric tumor may present in a metachronous or synchronous fashion. Less common associations have been ascribed to chronic inflammatory or scarring conditions such as in the setting of burns, so called Marjolin’s ulcer, osteomyletic sinuses, and lichen sclerosis et atrophicus, among others. The typical clinical presentation entails a rapidly growing keratotic papule or shallow ulcer on an exposed anatomic site in the elderly. These tumors may be broadly divided into intraepithelial malignancy and invasive tumors. The intraepithelial form synonymously referred to as Bowen’s disease or squamous cell carcinoma-in-situ, may histologically present in the guise of transepidermal keratinocytic dysplasia or as scattered dysplastic (pagetoid) keratinocytes found throughout all levels of the epithelium and extending into adjacent adnexal epithelium. These forms of the disease may exist in continuity with focal keratinocytic dysplasia confined to the basilar layer of the epithelium (actinic keratosis) or focal to full-thickness dysplasia without adnexal extension (bowenoid actinic keratosis). The relationship of these lesions to squamous cell carcinoma remains contentious, particularly in regard to their potential as precursors of SCC. Invasive squamous carcinoma can be histologically and prognostically stratified. Prognostic subcategorization came been accomplished on the basis of their degree of differentiation (well, moderate and poor) with increasing de-differentiation representative of a worse prognosis. Additional prognostic attributes which may be sought after include the depth of dermal invasion, the presence of vascular permeation or perineural extension. Deeper dermal extension, vascular permeation and perineural involvement have all been shown to portend a worse outcome. Histologic variants include a pigmented form associated with benign intra-tumoral melanocytes, an acantholytic form with dyshesive neoplastic keratinocytes, a spindled form which may be readily confused with melanoma or other spindled tumors, a lymphoepithelioma type with a rich endowment of lymphocytes, and a warty-like verrucous variant.
Epidemiology
Second most common skin cancer, rare in the dark-skinned races
Etiology
Ultraviolet light, HPV infection
Pathogenesis
p53 tumor suppressor gene mutation
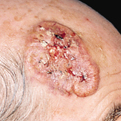
Clinical
Rapidly growing keratotic papule or shallow ulcer in sun-exposed site of elderly
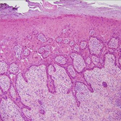
Histology
In situ lesions with full thickness or pagetoid scatter of dysplastic keratinocytes, invasive infiltrating keratinizing neoplasm may be pigmented, warty (verrucous), acantholytic, heavily inflamed (lymphoepithelioma) or spindled
Bibliography
1. Lohmann C, Solomon A. Clinicopathologic variants of cutaneous squamuos cell carcinoma. Adv Anat Pathol 2001; 8: 27. 2. Alam M, Ratner D. Cutaneous squamous cell carcinoma. N Engl J Med 2001; 344: 975. 3. Epsteim J. Photocarcinogenesis, skin cancer, and aging. J Am Acad Dermatol 1983; 9: 487.
Download PDF
![]() Squamous Cell Carcinoma
Squamous Cell Carcinoma