Merkel Cell Carcinoma

General Information
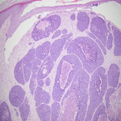
Merkel cell carcinoma, otherwise referred to a trabecular carcinoma, is an uncommon yet deadly dermal neoplasm potentially confused with other cutaneous neoplasms. Like its more common cancerous counterparts in the skin, it most commonly occurs in the sun-exposed sites of elderly patients and is predisposed for by ionizing radiation as well as waning immunity. Its histogenesis is speculated to derive from the slow-adapting dermal neuroendocrine mechanoreceptor known as the merkel cell. The pathology is varied consisting of one or more of three histologic archetypes; 1.) diffuse permeation of the dermis, 2.) large rectangular-shaped trabeculae or as 3.) rounded discrete foci. The latter tumoral disposition is most apt to be confused by the non-cognezetti as basal cell carcinoma. The cellular constituency consists of a uniform population of closely opposed cells with scanty cytoplasm and nuclei with indistinct nucleoli. Subtle histologic features which should allow for its distinction in most cases entail: 1.) lack of peripheral tumoral palisading, 2.) lack of tumor-stromal clefting; 3.) increased numbers of mitoses and apoptotic nuclei; 4.) a diffuse nuclear chromatin pattern; 5.) cellular apposition or molding 6.) the presence of tumoral crush artifact. Immunostaining is a useful diagnostic adjunct with particular emphasis placed upon the pattern of cytokeratin immunostaining (dot-like with merkel cell, diffuse in the other carcinomas), neuroendocrine differentiation (synaptophysin, chromogranin positivity) and the absence of lymphoid markers (i.e CD-45 seen in lymphomas) or lung markers (thyroid transcription factor for metastatic oat cell carcinoma). The clinical presentation of these neoplasms is non-descript mimicking other carcinomas including basal cell and squamous cell carcinomas. The biologic course of these neoplasms is extremely aggressive with a propensity to locally recur and to metastasize through a hematogenous or lymphatic route. The overall mortality rate is 50% at 5-years with the most important prognosticators being tumor stage at the time of diagnosis, including the absence of lymph node metastases or evidence of systemic disease. The treatment involves excisional therapy for localized disease and combinations of radiotherapy and chemotherapy for systemic disease. The most effective mode of treatment for localized disease is contentious. Given the aggressive nature of the disease with priority given to its extirpation in lieu of tissue preservation, the subtlety of the tumor cells at the margins or fringe of the tumors and the limitations imposed by the frozen technique, a compelling argument can be marshaled against treating these neoplasms with frozen section margin control or MOHS surgery. However, the cosmetically sensitive locale of these tumors and successful experience in regards to the management Merkel cell carcinoma with the MOHS technique offer a contravening view. These antithetical views may be reconciled by a pra
Epidemiology
Uncommon, elderly with equal gender distribution
Etiology
Ultraviolet light, immunosupression, polyoma virus
Pathogenesis
Clinical
Histology
Bibliography
1. Morgan, MB. Merkel Cell Carcinoma. In Deadly Dermatologic Diseases. Morgan M.B., ed. Springer, New York, 2007. 2. Boyer J, Zitelli J, Brodland D, et al. Local control of primary Merkel cell carcinoma : Review of 45 cases treated with Mohs micrographic surgery with and without adjuvant radiation. JAAD 2002; 47: 885. 3. O’Connor W. Merkel cell carcinoma . Comparison of Mohs micrographic surgery and wide excision. In eighty-six patients. Dermatol Surg 1997; 23: 929.
Download PDF
![]() Merkel Cell Carcinoma
Merkel Cell Carcinoma