Sebaceous Carcinoma

General Information
Sebaceous carcinoma otherwise referred to as meibomian gland carcinoma is an uncommon yet aggressive sebaceous neoplasm that occurs within the eyelid. Although histologically identical tumors may occur within any sebaceous gland containing cutaneous site, they do not pursue as an aggressive biologic course and given their less sensitive anatomic location may not require the use of tissue sparing frozen section/Mohs resection treatment. The meibomian glands are modified sebaceous glands devoid of an interposed follicle found in association with the upper and lower tarsal eyelid plates. These glands are distinct from the eyelash-associated sebaceous glands of Zeis or similar glands associated with caruncle or surface vellus hairs. The pathogenesis of these neoplasms is unknown although ultraviolet and ionizing irradiation have been implicated in their development. Sebaceous carcinoma is also associated with the Muir-Torre DNA-mismatch repair defect syndrome. Unlike sporadic cases seen in the elderly, those tumors that arise in conjunction with this syndrome tend to afflict the middle-aged patient. The microscopic features are distinct and consist of the demonstrated presence of sebocytic differentiation. The latter change consists of neoplastic cells possessing enlarged nuclei with prominent nucleoli and most importantly, lipid cytoplasmic vacuoles that appear as multiple rounded clear areas or as diagnostic areas of staining with lipid stains on fresh frozen biopsy tissue specimens. Fat staining with agents such as Oil red-O cannot be performed on formalin fixed or processed tissues, instead the diagnosis relies upon the demonstration of the sebocytes or of sebaceous differentiation with the aid of immunohistochemical staining. The latter technique can be employed on frozen or formalin-fixed tissues and consists of epithelial membrane antigen (EMA) or carcinoembryonic antigen (CEA) or cytokeratin -7 (CK-7) immunopositvity. These immunostains should not decorate the cells comprising routine squamous cell or basal cell malignancies. Sebaceous carcinoma typically presents as invasive infiltrative neoplasm or rarely as an intraepidermal neoplasm showing pagetoid spread simulating Bowen’s or Paget’s disease. The clinical appearance of these lesions is non-descript being similar to their more common basal cell or squamous cell counterparts. Approximately 25% of tumors will have metastasized to regional lymph nodes at the time of diagnosis. The prognosis of patients with metastatic disease drops to 50% at 5 years.
Epidemiology
Uncommon, approximately 1/2 occur on eyelids, elderly with equal gender, syndromic female younger.
Etiology
Derive from Meibomian glands, other sebaceous glands, assoc. with XRT and Muir-Torre Syndrome.
Pathogenesis
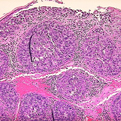
Pagetoid or invasive basaloid or squamous cells with sebocytic cells showing clear cytoplasmic vacuoles.
Clinical
Non-descript ulcerating papule, may be yellow in appearance or involve both eyelids.
Histology
Bibliography
1. Nelson B, Hamlet K, Hillard M, et al. Sebaceous carcinoma. JAAD 1995; 33: 1. 2. Rao N, Hidayat A, McClean I, et al. sebaceous carcinoma of the ocular adnexae: a clinicopathalogic study of 104 cases, with 5 year follow up. Hum Pathol 1982; 13: 113. 3. Schwartz R, Torre D. The Muir-Torre syndrome: a 25-year retrospect. JAAD 33: 90.
Download PDF
![]() Sebaceous Hyperplasia
Sebaceous Hyperplasia