

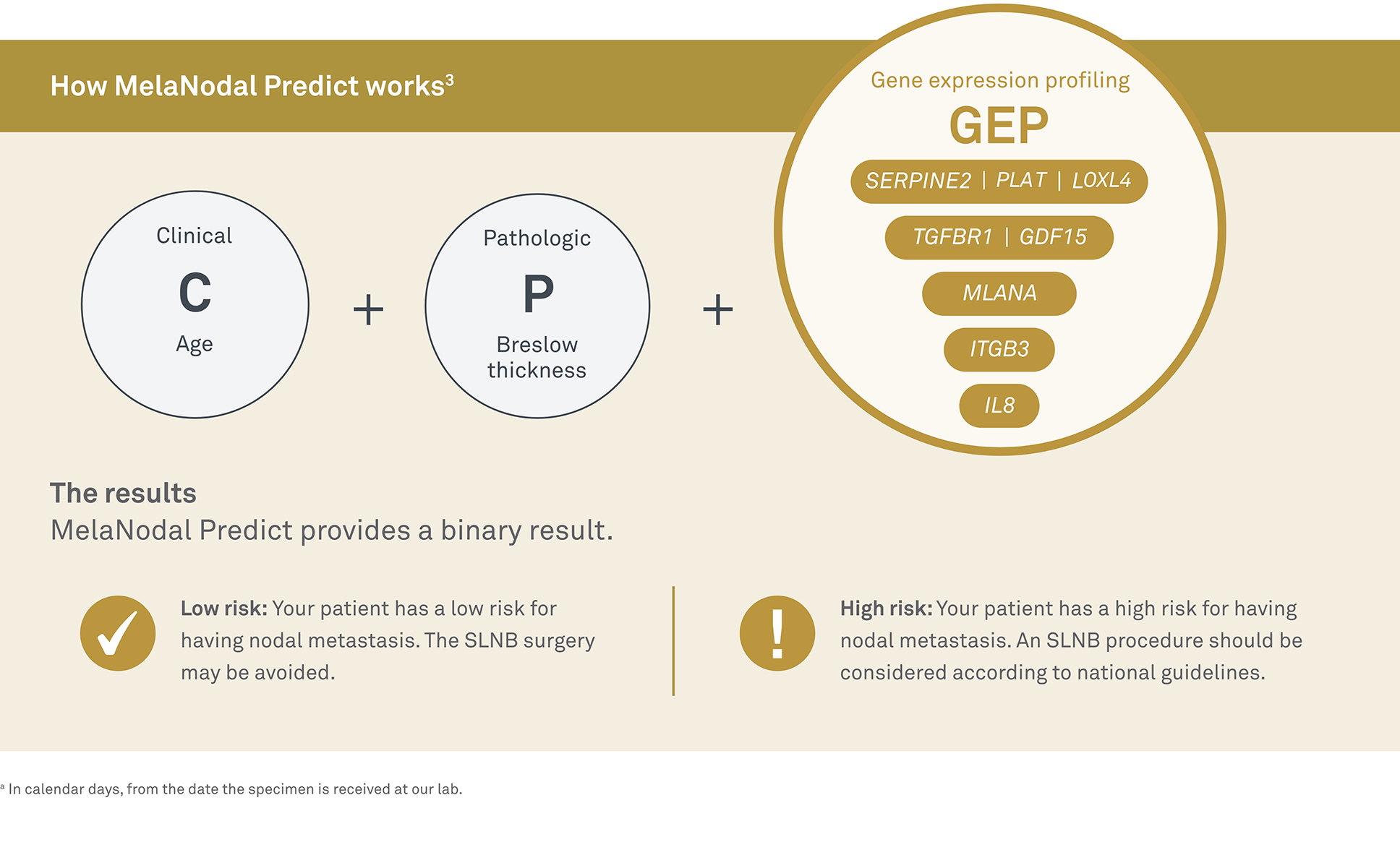
MelaNodal Predict™ is an innovative gene expression profiling (GEP) assay that assesses a patient’s tumor genomics alongside clinicopathologic features to identify their level of risk for SLN metastasis. With results available in 3-5 days,a the assay objectively qualifies which patients are at a low level of risk for nodal metastasis and who may be able to avoid undergoing SLN biopsies.

According to the International Journal of Dermatology, ~80% of melanoma patients undergoing sentinel lymph node biopsy (SLNB) have no evident nodal metastasis and meet the definition of “low risk.”2-4
With the gene expression profiling (CP-GEP) used in MelaNodal Predict, clinicians can evaluate risk more precisely. In one study, when CP-GEP was used to retroactively reevaluate high- and low-risk patients, SLNB did not improve outcomes for as many as 51% of patients with low risk for metastasis. Forgoing SLNB might have helped these patients avoid the invasive procedure, along with as many as 59% of SLNB-associated complications like lymphedema and hematoma.2-4
Make more-informed treatment decisions to improve care for patients with cutaneous melanoma
Clinical studies support the effectiveness of MelaNodal Predict:
CP-GEP technology used in MelaNodal Predict may reduce the need for SLNB by 51% and associated complications (such as lymphedema or hematoma) by 59%2
Patients identified as low risk had significantly higher 5-year survival rates, which may justify forgoing SLNB and associated complications2,3

Significant cost savings, where patients identified as low-risk via CP-GEP testing were recommended to undergo wide local excision (WLE) of the primary tumor at $2,066, versus $11,976 for a SLNB and WLE5

CP-GEP identified as high risk, which may indicate survival-extending adjuvant therapy and closer monitoring2
Our dermatopathology and hematopathology fellows, with their clinical and anatomic pathology expertise, equip us with knowledge of common and rare intersections between dermatology and hematology.
References
1. Swetter SM, Thompson JA, Albertini MR, et al. NCCN Guidelines® insights: melanoma: cutaneous, version 2.2021: featured updates to the NCCN Guidelines. J Natl Compr Cancer Netw. 2021;19(4): 364-376.doi:10.6004/jnccn.2021.0018
2. Hieken TJ, Sadurni MB, Quattrocchi E, et al. Using the Merlin assay for reducing sentinel lymph node biopsy complications in melanoma: a retrospective cohort study. Int J Dermatol. 2022;61(7):848-854.doi:10.1111/ijd.16056
3. Bellomo D, Arias-Mejias S, Ramana C, et al. A model combining tumor molecular and clinicopathologic risk factors predicts sentinel lymph node metastasis in primary cutaneous melanoma. JCO Precis Oncol. 2020;4:319-334. doi:10.1200/PO.19.00206
4. Amaral T, Sinnberg T, Chatziioannou E, et al. Identification of stage I/II melanoma patients at high risk for recurrence using a model combining clinicopathologic factors with gene expression profiling (CP-GEP). Eur J Cancer. 2023;182:155-162. doi:10.1016/j.ejca.2022.12.021
5. Thao V, Dholakia R, Moriarty JP, et al. Cost evaluation of the Merlin assay for predicting melanoma sentinel lymph node biopsy metastasis. Int J Dermatol. 2023;62(1): 56-61. doi:10.1111/ijd.16515